- Definition
- Etiology
- Pathogenesis
- Pathology
- Epidemiology
- Management & Treatment
- Prevention
- Complications
- Prognosis
- Research Frontier
- Clinical Case Studies
- Study Questions
[Acute rheumatic fever (ARF) is a nonsuppurative sequela of group A Streptococcus (GAS) pharyngitis that occurs two to four weeks following infection.]
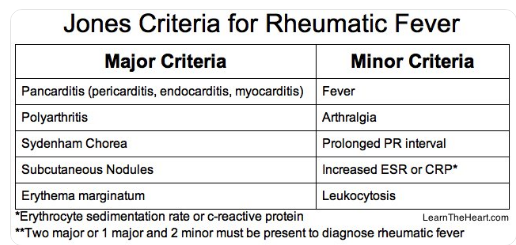
●The five major manifestations (major Jones Criteria) of ARF are migratory arthritis (predominantly involving the large joints), carditis and valvulitis (eg, pancarditis), central nervous system involvement (eg, Sydenham chorea), erythema marginatum, and subcutaneous nodules. The four minor manifestations (minor Jones Criteria) are arthralgia, fever, elevated acute phase reactants, and prolonged PR interval on electrocardiogram. (See 'Acute illness' above.)
●The diagnosis of ARF is established on clinical grounds. The probability of ARF is high in the setting of GAS infection followed by two major criteria or one major and two minor criteria. The criteria are modified slightly for patients in moderate- to high-risk populations. (See 'Diagnosis' above.)
●Arthritis usually is the earliest symptomatic manifestation of ARF. The natural history consists of inflammation affecting several joints in quick succession with overlapping onset, giving the appearance that the disease "migrates" from joint to joint. Joint pain usually is more prominent than objective signs of inflammation and is almost always transient. (See 'Arthritis' above.)
●ARF causes a pancarditis, affecting the pericardium, epicardium, myocardium, and endocardium, with valvulitis being the most common clinical presentation. However, the carditis can be subclinical. (See 'Carditis' above.)
●Sydenham chorea (also known as chorea minor or "St. Vitus dance") is a neurologic disorder consisting of abrupt, nonrhythmic, involuntary movements; muscular weakness; and emotional disturbances. (See 'Sydenham chorea' above.)
●Erythema marginatum is an evanescent, pink or faintly red, nonpruritic rash involving the trunk and sometimes the limbs but not the face (picture 1 and picture 2). The lesion extends centrifugally, with return of the skin in the center to a normal appearance. (See 'Erythema marginatum' above.)
●Subcutaneous nodules are firm, painless lesions ranging from a few millimeters to 2 cm in size (picture 3). The nodules are usually located over a bony surface or prominence or near tendons (usually extensor surfaces) and are usually symmetric. (See 'Subcutaneous nodules' above.)
●The most common sequela of ARF is rheumatic heart disease (RHD). RHD usually occurs 10 to 20 years after the original illness and is the most common cause of acquired valvular disease in the world. (See 'Rheumatic heart disease' above and "Clinical manifestations and diagnosis of rheumatic heart disease".)
●Some cases of arthritis occurring after a streptococcal infection are not accompanied by sufficient additional Jones Criteria to meet diagnostic requirements for ARF. This disorder has been called poststreptococcal reactive arthritis (PSRA). (See 'Poststreptococcal reactive arthritis' above.)
Acute rheumatic fever (ARF) results from the body’s autoimmune response to a throat infection caused by Streptococcus pyogenes, also known as the group A Streptococcus bacteria.1

Pathogenesis of carditis in acute rheumatic fever (VCAM1: Vascular cell adhesion molecule 1). Figure reproduced with permission from (Carapetis, et al., 2016).
The development of ARF occurs approximately two weeks after S. pyogenes infection (Gewitz, et al., 2015).
The clinical manifestations and symptoms of ARF can be severe and are described in the Revised Jones Criteria (Gewitz, et al., 2015). Symptoms of ARF can include polyarthritis, carditis, chorea, the appearance of subcutaneous nodules, and erythema marginatum or a rash associated with ARF (Gewitz, et al., 2015; Martin, et al., 2015). These symptoms usually require patients to be hospitalized for two to three weeks, during which time the outward symptoms resolve, but the resultant cardiac damage may persist. With repeated S. pyogenes pharyngitis infections, ARF can recur and cause cumulative damage to the heart valves (Martin, et al., 2015).
Acute rheumatic fever is an inflammatory syndrome. It is associated with a high incidence of chronic valvular heart disease
Nodules - These resemble histologically the Aschoff nodules seen in the heart.
Eradication of Group A Streptococcus from the oropharynx.
Penicillin is the antibiotic of choice. Oral therapy should be continued for at least 10 days.
Dose:
Penicillin-allergic patients can be treated with cephalosporins or macrolide antibiotics.21
Due to the high rate of recurrence in previously affected people, antibiotic prophylaxis is recommended, especially in endemic areas.
Anti-inflammatory medication
The acute inflammatory process is largely treated symptomatically, including bed rest during the early phase of the syndrome.48
Anti-inflammatory medications including salicylates and nonsteroidal agents are effective for the arthritis, fever, and arthralgia.
[However, salicylates alone have not been shown to be effective in decreasing the incidence of rheumatic heart disease after ARF. ]
Corticosteroids are believed to be beneficial in the treatment of carditis; though this has never been shown in a randomized controlled trial.
Approximately 80% of patients who fulfill the criteria for this disorder recover spontaneously.
Content 13
Content 11